Air pollution in Kawempe Division of Kampala, Uganda
Introduction
The wellness effects of air pollution have been widely documented and assessed largely in North America and Europe, nevertheless air pollution in low- and middle-income states pose a great public wellness load that has non been decently assessed ( 1–6 ). All right particulate affair comprised of atoms of width 2.5g or less ( PM2.5) has been associated with mortality due to the development of cardiovascular or respiratory diseases and lung malignant neoplastic disease ( 3 ).
In the Kawempe Division in Kampala ( Uganda ) measurings of PM2.5from December 2013 and January 2014 were found to be above guideline bounds of the World Health Organization ( WHO ) bespeaking the demand for a consistent exposure appraisal of the air pollution and its wellness load in Uganda ( 7,8 ).
Order custom essay Air pollution in Kawempe Division of Kampala, Uganda with free plagiarism report
 450+ experts on 30 subjects
450+ experts on 30 subjects
 Starting from 3 hours delivery
Starting from 3 hours delivery
Hazard Identification
Acute events of smog in the Meuse vale in Belgium and in London in 1933 and 1952, severally were among the first events that indicated the association between air pollution and mortality ( 9,10 ). More late epidemiologic surveys quantified the effects of chronic and ague exposures to poisons such as a particulate affair, ozone, or benzine on wellness ( 3,11,12 ). More specifically PM2.5exposure has been associated with inauspicious wellness results in big epidemiologic surveys in assorted scenes ( 8,13 ).
Chronic effects of exposure to particulate affairs have been studied in prospective cohort surveys with big sample sizes and long follow-up periods in assorted locations such as the US, Canada, Europe, and China ( 2,4,5 ). The first survey that associated cardiorespiratory and lung malignant neoplastic disease mortality with PM2.5was published in 1993 by Dockery et Al ( 3 ).
In this first appraisal informations from six metropolia with changing degrees of air pollution and mortality from cardiorespiratory diseases, lung malignant neoplastic disease, all causes of mortality and mortality from all other causes except cardiorespiratory diseases or lung malignant neoplastic disease was investigated. Following up on the “six metropolis studies” Laden et Al. in 2006 reported on the association between cardiovascular diseases ( CVD ) mortality, lung malignant neoplastic disease, and respiratory upsets ( 14 ). Following up on the same cohort and reanalyzing the information Lepeule et Al. in 2012 besides confirmed the association between CVD and lung malignant neoplastic disease mortality with PM2.5exposures ( 15 ).
In 2002, Pope et Al. besides reported the consequences of a larger cohort with PM2.5measurings of 51 metropolitan countries in the US, reasoning besides that there is increased hazard of mortality at 4 %, 6 % and 8 % from all causes, CVD, and lung malignant neoplastic disease, severally with each 10?g/m3addition in PM2.5( 4 ). Similar consequences were besides reported in the Canadian survey of Crouse et al. , 2012 in a cohort of 2.1 million Canadian grownups ( 16 ).
All these surveies set the scene for a comprehensive wellness hazard appraisal of PM2.5. They provided cohesive and timely consequences from dependable beginnings on the fluctuations PM2.5and mortality fulfilling Hill’s standards.
Exposure Appraisal
Kampala, the capital of Uganda has a population of about 1,500,000, it is the 2neodymiummost thickly settled territory in the state ( 17 ). The Kawempe division of Kampala is located in the North of the metropolis and has a population of 338,312, with an estimated 84,240 above the age of 30 old ages ( 17 ). Measurement of ambient PM2.5degrees took topographic point two years during winter 2012-2013 in the country of Mperewre of the Kawempe Division and they were reported as portion on a pilot survey published in 2014 ( 7 ).
The mean Autopsy2.5concentration for the topographic point measurements was 104.3?g/m3. It besides exceeds both the one-year and 24-hour WHO guideline values that are set at 10?g/m3and 25?g/m3, severally, and antecedently reported measurings in developed states ( 8 ). The mensural PM2.5degrees are nevertheless consistent with measurements in other developing states.
Data from Asiatic metropolis suggest that the high Autopsy2.5concentrations are nonrare in developing scenes where monitoring is non routinely conducted. Harmonizing to the 2010 study of the Health Effects Institute on outdoor air pollution in the underdeveloped states of Asia the degrees of PM2.5can be every bit high as 150?g/m3( 6 ).
In the same study, for illustration, in Shenzhen and Guangzhou, in China, 24-hour mean summer concentrations of PM2.5were 35?g/m3Autopsy2.5was every bit high as 97.5?g/m3. Exposure appraisal of PM2.5effects on mortality in the Kawempe Division is hindered by the deficiency of one-year norm values that would reflect fluctuations in air pollution. However given the features of the country, where a landfill is located and the tendency for increased urbanization in Uganda and its deductions ( i.e. increased traffic etc ) the high Autopsy2.5degrees in Mperewre may reflect the norm of PM2.5degrees in the location ( 18,19).
Within the range of the present exposure appraisal, we have based on the premise that the mean of the available topographic point measurements reflects the average PM2.5degrees in the Kawempe division of Kampala. Based on the handiness of information we can non be certain about the PM2.5concentrations fluctuate in the country over clip and the derived decision might be over- or undervaluing the existent wellness effects of PM2.5wellness effects.
Table 1 Autopsy2.5concentrations and meteoric parametric quantities on the years that measurement took topographic point harmonizing to Schwander et al. , 2014.
| December 31, 2012 | January 2, 2013 | |
| Autopsy2.5concentrations (?g/m3) | 104.9 | 103.7 |
| Average concentration (?g/m3) | 104.3 | |
| Meteorologic parametric quantities | ||
| Average temperature (0C ) [ min, soap ] | 22.2 [ 18.9, 25.0 ] | 24.4 [ 20.6, 27.8 |
| Dew point temperature (0C ) | 18.9 | 20.0 |
| Mean wind velocity ( kilometers per hour ) [ max ] | 8.1 [ 16.1 ] | 8.1 [ 19.3 ] |
Exposure-Response Analysis
The exposure-response relationships between PM2.5and mortality from CVD and lung malignant neoplastic disease have been antecedently studied in US populations by Laden et Al. ( six metropolis studies, follow-up ) and by Pope et Al. ( 4,14,22 ). In the survey of Laden CVD and lung, malignant neoplastic disease decreases were associated with exposure to PM2.5( 14 ). Specifically a 10?g/m3addition in the mean Autopsy2.5was associated with the comparative hazard ( RR ) of 1.28 ( 1.13-1.44, 95 % CI ) for CDV mortality and a RR of 1.27 ( 0.96-1.69, 95 % CI ) for lung malignant neoplastic disease mortality.
In the survey of Pope et al. , 2002 for the same PM2.5incremental alteration addition in lung malignant neoplastic disease mortality was estimated at 8 % ( 4 ). Both surveys, the 1993 survey of the six metropolia and the Lepeule’s follow up have established the association between increased exposure to PM2.5and increased hazard for CVD and lung malignant neoplastic disease mortality. The form of the exposure-response map nevertheless is nonadditive in all doses nor does it hold the same form for both results.
The exposure-response map of mortality from CVD starts steep in low exposures and going flattered with increasing concentrations ( 22 ). In the instance of the lung, malignant neoplastic disease mortality the exposure-response map is more additive and it is, as expected, more influenced by confounders ( i.e. smoke ) ( 22 ).
Additionally in all the aforesaid surveies the exposure-response maps have been established based on the effects of low exposures, normally below 50?g/m3. In Uganda, the age-adjusted mortality rate from lung malignant neoplastic disease is 2.7 among males and 2.4 among females ( per 100,000 ) while the same index for CVD is 276.7 and 250.7 per 100,000 population ( males and females, severally ) ( 20,21 ).
In order to gauge the figure of CVD and lung malignant neoplastic disease deceases attributed to 104?g/m3of ( assumed ) one-year exposure we will be based on the exposure-response maps for CVD and lung malignant neoplastic disease mortality developed by Pope et al, 2011 that were derived from a prospective cohort of 1.2 million grownups ( & gt; 30 old ages old ) and old surveys in the US which accounted for assorted confounders of exposure.
They estimated the RR associated with different degrees of PM2.5exposure accounting for ambient air pollution, active coffin nail smoke, and secondhand smoke to gauge the day-to-day norm inhaled dosage of PM2.5. The RR for each of the two results ( CVD and lung malignant neoplastic disease mortality ) was so calculated with the power map: RR=1+? ( dosage )? This corresponds to a nonlinear monotone map for which at zero doses the RR is equal to 1.
Table 2 Exposure appraisal information
| Population features( 17 ) | ||||
| Males | Females | Entire | ||
| Kawempe Division | 159,8 | 178,512 | 338,312 | |
| Population above 30 old ages old ( 24.9 % * ) | 39,79 | 44,449 | 84,24 | |
| Kampala | 722,638 | 793,572 | 1,516,210 | |
| Entire population | 16,935,456 | 17,921,357 | 34,856,813 | |
| Age-standardized decease rates per 100000( 20,21 ) | ||||
| Cardiovascular diseases | 276.7 | 250.7 | ||
| Lung malignant neoplastic disease | 2.7 | 2.4 | ||
| The entire figure of deceases in Kawempe territory for the those & gt; 30 old ages old | ||||
| Cardiovascular diseases | 110 | 111 | 222 | |
| Lung malignant neoplastic disease | 1 | 1 | 2 | |
| RR estimations for both genders ( for the dosage of PM2.5104?g/m3) | Attributable hazard fraction | Number of instances attributed to PM2.5 | ||
| Cardiovascular diseases | RR=1+0.2685 ( dosage )0.2730 | 1.95 | 0.49 | 108 |
| Lung malignant neoplastic disease | RR=1+0.3195 ( dosage )0.7433 | 11.09 | 0.91 | 2 |
Hazard Word picture
With an estimated RR of 1.95 for CVD mortality due to PM2.5degrees of 104?g/m3the PM2.5-associated mortality instances in the entire population above 30 old ages old of Kawempe Division is about 108 ( Table 2 ). The age-standardized mortality rate for CVD – the primary wellness result that has been associated with increased air pollution – in Uganda is comparatively high contrary and future research is needed to decently gauge the fraction of instances attributed to air pollution which was comparatively high in this study ( 0.49, ( Table 2 ).
As expected given the to the low mortality rate of lung malignant neoplastic disease in the country and the fact it is confounded by other factors that could non be assessed in ( i.e. smoking ) we can non properly measure the impact of PM2.5on the figure of lung malignant neoplastic disease deceases in Kawempe Division.
For the present analysis, the information used was compiled from assorted beginnings. Population estimations were taken from the probationary study on the 2014 nose count. Lung malignant neoplastic disease and CVD age-standardized mortality rates were taken from GLOBOCAN and the WHO, several. Therefore all computations are based on the premise that for 2014 of Kawempe Division the mortality rates are the same as the last reported in the aforesaid beginnings.
The fact that there is the information might not reflect the decently the features of the population is an of import restriction of this appraisal. Along with the fact that hazard estimations were based on surveys of lower Autopsy2.5degrees. Future research needs to be based on seasonably collected information and hazard theoretical accounts that account for the high exposures.
Reference
- Katsouyanni K, Rimm EB, Gnardellis C, Trichopoulos D, Polychronopoulos E, Trichopoulou A. Reproducibility and comparative cogency of an extended semi-quantitative nutrient frequency questionnaire utilizing dietetic records and biochemical markers among Grecian school teachers.
- Raasch-Nielsen O, Andersen ZJ, Beelen R, Somali E, Stafoggia M, Weinmayr G, et Al. Air pollution and lung malignant neoplastic disease incidence in 17 European cohorts: prospective analyses from the European Study of Cohorts for Air Pollution Effects ( ESCAPE ). The Lancet Oncology. 2013 Aug ; 14 ( 9 ) :813–22.
- Dockery DW, Pope CA, Xu X, Spengler JD, Ware JH, Fay ME, et Al. An Association between Air Pollution and Mortality in Six U.S. Cities. New England Journal of Medicine. 1993 Dec 9 ; 329 ( 24 ) :1753–9.
- Pope III CA. Lung Cancer, Cardiopulmonary Mortality, and Long-run Exposure to Fine Particulate Air Pollution. JAMA. 2002 Mar 6 ; 287 ( 9 ) :1132.
- Cao J, Yang C, Li J, Chen R, Chen B, Gu D, et Al. Association between long-run exposure to outdoor air pollution and mortality in China: A cohort survey. Journal of Hazardous Materials. 2011 Feb 28 ; 186 ( 2–3 ) :1594–600.
- HEI International Scientific Oversight Committee. Outdoor Air Pollution and Health in the Developing Countries of Asia: A Comprehensive Review. Boston, MA: Health Effects Institute; 2010.
- Schwander S, Okello CD, Freers J, Chow JC, Watson JG, Corry M, et Al. Ambient Particulate Matter Air Pollution in Mpererwe District, Kampala, Uganda: A Pilot Study. J Environ Public Health [ Internet ]. 2014 [ cited 2015 Feb 26 ] ; 2014. Available from: hypertext transfer protocol: //www.ncbi.nlm.nih.gov/pmc/articles/PMC3945229/
- WHO | Air quality guidelines - planetary update 2005 [ Internet ] . WHO. 2015 [ cited 2015 Mar 5 ] . Available from: hypertext transfer protocol: //www.who.int/phe/health_topics/outdoorair/outdoorair_aqg/en/
- Bell ML, Davis DL. Reappraisal of the deadly London fog of 1952: fresh index of ague and chronic effects of acute exposure to air pollution. Environ Health Perspect. 2001 Jun; 109 ( Suppl 3 ):389–94.
- Nemery B, Hoet PH, Nemmar A. The Meuse Valley fog of 1930: an air pollution catastrophe. The Lancet. 2001 Mar ; 357 ( 9257 ) :704–8.
- Kheirbek I, Wheeler K, Walters S, Kass D, Matte T. PM2.5 and ozone wellness impacts and disparities in New York City: sensitiveness to the spacial and temporal declaration. Air Qual Atmos Health. 2012 Oct 12 ; 6 ( 2 ) :473–86.
- Savitz DA, Andrews KW. Review of epidemiologic grounds on benzine and lymphatic and hematopoietic malignant neoplastic diseases. Am J Ind Med. 1997 Mar 1; 31 ( 3 ):287–95.
- US EPA O. Particulate Matter | Air & A ; Radiation | US EPA [ Internet ] . 2013 [ cited 2015 Mar 9 ] . Available from: hypertext transfer protocol: //www.epa.gov/pm/
- Laden F, Schwartz J, Speizer FE, Dockery DW. The decrease in Fine Particulate Air Pollution and Mortality. Am J Respir Crit Care Med. 2006 Mar 15 ; 173 ( 6 ) :667–72.
- Lepeule J, Laden F, Dockery D, Schwartz J. Chronic Exposure to Fine Particles and Mortality: An Drawn-out Follow-up of the Harvard Six Cities Study from 1974 to 2009. Environmental Health Perspectives. 2012 Mar 28 ; 120 ( 7 ) :965–70.
- Crouse DL, Peters PA, new wave Donkelaar A, Goldberg MS, Villeneuve PJ, Brion O, et Al. Hazard of Nonaccidental and Cardiovascular Mortality in Relation to Long-term Exposure to Low Concentrations of Fine Particulate Matter: A Canadian National-Level Cohort Study. Environmental Health Perspectives. 2012 Feb 7 ; 120 ( 5 ) :708–14.
- UBOS. National Population and Housing Census 2014 - Probationary consequences [ Internet ]. Uganda Bureau of Statistics; 2014 Nov. Available from hypertext transfer protocol: //www.ubos.org/onlinefiles/uploads/ubos/NPHC/NPHC 2014 PROVISIONAL RESULTS REPORT.pdf
- Mwiganga M, Kansiime F. The impact of Mpererwe landfill in Kampala – Uganda, on the environing environment. [ Internet ] . Makerere University - College of Agricultural and Environmental Sciences. 2012 [ cited 2015 Mar 9 ] . Available from: hypertext transfer protocol: //caes.mak.ac.ug/research/research-publications/141-publications-for-2005/820-the-impact-of-mpererwe-landfill-in-kampala-uganda-on-the-surrounding-environment.html
- Mwiganga M, Kansiime F. The impact of Mpererwe landfill in Kampala–Uganda, on the environing environment. Physics and Chemistry of the Earth, Parts A/B/C. 2005 ; 30 ( 11–16 ) :744–50.
- WHO. Noncommunicable Diseases ( NCD ) Country Profiles - Uganda [ Internet ] . 2014 [ cited 2015 Mar 9 ] . Available from: hypertext transfer protocol: //www.who.int/nmh/countries/uga_en.pdf? ua=1
- Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C, et Al. Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11 [ Internet ]. GLOBOCAN 2012 v1.0. 2013 [ cited 2015 Mar 5 ] . Available from: hypertext transfer protocol: //www.who.int/phe/health_topics/outdoorair/outdoorair_aqg/en/
- Pope CA, Burnett RT, Turner MC, Cohen A, Krewski D, Jerrett M, et al. Lung Cancer and Cardiovascular Disease Mortality Associated with Ambient Air Pollution and Cigarette Smoke: Shape of the Exposure–Response Relationships. Environmental Health Perspectives. 2011 Jul 19 ; 119 ( 11 ) :1616–21.
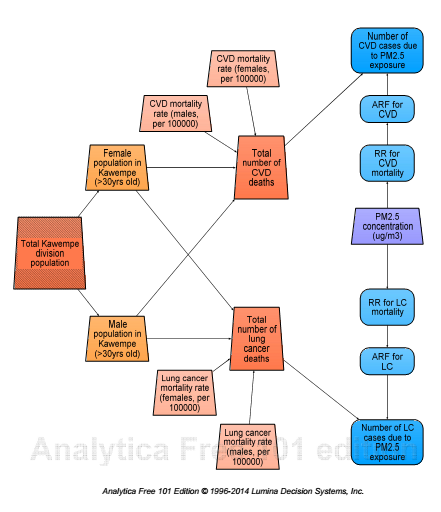
Appendix – Analytica theoretical account
Cite this Page
Air pollution in Kawempe Division of Kampala, Uganda. (2017, Jul 07). Retrieved from https://phdessay.com/air-pollution-in-kawempe-division-of-kampala-uganda/
Run a free check or have your essay done for you
